Eline van den Broek-Altenburg, an assistant professor at the Larner College of Medicine, University of Vermont, and Adam Atherly, a professor and director of the Center for Health Services Research at the Larner College of Medicine, University of Vermont have produced a short analysis titled “Economic Cost of Flattening the Curve.”
It’s interesting and valuable, but it’s mis-titled. The best part is their analysis of the benefit of saving lives. Even that, though, is misleading because they write as if their implicit assumption is that implementing a plan would save all the lives that would have been lost to the COVID-19 disease. NO ONE believes that.
Still, let’s go on. They point out some very interesting facts about the data from Italy, facts that have, in most of what I’ve seen, not been given their due. The most important one is this:
The Italian National Health Institute pegged the median age of death from COVID-19 in Italy at 80.5. This is consistent with early data from the United States.
They also say that there’s good reason to think that the mean age of death for the above is close to the median.
If you’ve ever seen one of these studies, you know where they’ll go next: calculate the number of extra life years saved by a death averted. They write:
The average 80-year old in the United States has a life expectancy of about 9 years, suggesting that on average, a death averted will “buy” 9 extra years of life. In QALY-estimations, this number needs to be adjusted for the “quality of the years”. In Italy, 99% of deaths had an underlying pathology that needs to be incorporated in QALY adjustments. If we use diabetes as a reasonable proxy for the many chronic diseases, we would adjust the 9 years down to 7.8 years or QALYs. In other words: the average loss per person of quality-adjusted life years is 7.8.
QALY stands for Quality Adjusted Life Year. It’s what a lot of health economists use in estimating gains from various drugs, surgeries, changes in safety, etc.
Then they take an expected range of deaths of 200,000 to 1.7 million. Although only 2 weeks ago, I told my friend Charley Hooper that I expected at least 200,000 deaths, my own view now is that 200,000 is too high.
Then they multiply these deaths by 7.8 years to get 1.56 million to 13.26 million QALYs.
They next want to consider the cost of achieving the benefit of not having these deaths. Let me remind you, though, that many of the deaths have already happened and you can’t prevent all future deaths. So their measure necessarily overstates the benefits (assuming you buy the idea of QALYs) of any government policy.
Now let’s go to the even bigger mistake. They don’t measure the cost of the measures to reduce (or, they would have to say, end) deaths. No. What they do instead is look at the cost of the stimulus bill that Congress is considering. But wait. The stimulus bill isn’t aimed at preventing deaths. It’s aimed at compensating people for losses (along with some pork). So I found the rest of their analysis not that useful.
Here’s how to do it right.
Estimate the number of deaths averted, and the related number of QALYs saved, by implementing some government strategy. Then estimate the cost of this strategy. A rough measure would be, say, one month of average wages lost (minus 20% of wages lost, assuming people value the leisure somewhat) times the number of people losing these wages, plus one lost month of profits on businesses. That would be a much better measure, if the measure(s) cost about one month of output. I think it would be the same order of magnitude as their measure.
That means that their conclusion is understated. Here’s their conclusion:
In theory, if decision rules like cost effectiveness represent sensible approaches to making policy choices, health economists should be out front helping guide policy. Our calculations suggest that current strategies will be cost effective only if the predicted mortality rates are at the top of the predicted range and costs are at the bottom of the range – a combination of worst care / best case that is unlikely. Consideration of targeted mitigation strategies that minimize the economic cost while protecting the most vulnerable are warranted.
Why do I say their conclusion is understated? They’ve probably got the order of magnitude right on the cost side even though theirs is not an estimate of the cost. But by assuming all lives are saved, even those that are already lost, they may well have at least doubled the number of quality-adjusted life years saved.
HT2 Jerrod F. Anderson
READER COMMENTS
Ken P
Mar 25 2020 at 12:18am
I think the analysis misses other costly effects. I would expect the lost jobs and resulting financial distress to result in a higher ssuicide rate. This would likely be mostly young people so that cost would be high. It also does not include potential deaths from elderly people who become less healthy from being homebound due to the closure of places they like to go to.
David Henderson
Mar 25 2020 at 8:38am
You write:
That’s a really good point. And to make it directly comparable, a way we cost-benefit analysts would do it is not to put in on the cost side but to subtract those QALYs from the QALYs saved on the benefit side.
By the way, this is one data point, but a friend I was talking to last night told me a friend of a friend of his went kind of bonkers a few days ago and got paranoid about both the COVID-19 and feeling “locked up” in California, and murdered his brother. If it’s the COVID-19 that did it, that’s on one side of the balance sheet. If it’s the feeling of being locked up that did it, that’s on the other side. From the way my friend told the story, it seemed to me that it was mainly the latter.
Capt. J Parker
Mar 25 2020 at 9:37am
I had the same thought as Ken P – that mortality rates will rise during a recession and that you need to offset the reduction in COVID 19 deaths prevented by the number of deaths caused by an economic downturn. But, the magic of the internet quickly informed me that mortality rates drop during a recession and apparently this fact is well known even if the reason for it is not.
David Henderson
Mar 25 2020 at 1:24pm
It’s funny you mention that because it rang a dim bell in my head from a Sam Peltzman workshop at UCLA in 1973. Sam was presenting his preliminary results on the effect of making cars safer. He showed that there was no net reduction in fatalities of car occupants and there was an increase in fatalities of pedestrians and motorcyclists. All these, of course, were relative to predicted values based on other variables. One of the variables, if I recall correctly, was the unemployment rate. He expected the effect to go the opposite way: when times are good, real incomes are higher, safety is a normal good, yada, yada.
He found that it went the same way as in the paper you cite. Notice in that paper that the authors actually do find that relationship for vehicle fatalities.
Sam said he couldn’t understand it. He went through a lot of economics literature to try to figure out why and said that he couldn’t find anything. I even remember his next line: “So desperate was I to find an explanation that I even went to the sociology literature.” That got a guffaw from another Ph.D. student friend and me because of course, with our incredible sophistication at age 22 (me) and 24 (other friend), we knew that sociology had to be bunk. We hadn’t yet taken on Bryan Caplan’s view that you can learn a ton from other literatures. (I didn’t quite get that until my late 30s.)
Ken P
Mar 25 2020 at 10:06pm
Yes, it makes much more sense to subtract from the QALY’s saved. Thanks for the insight.
Another odd thing is the restrictions on elective surgeries. Elective surgeries pretty much collapsed prior to the restriction because it’s not the best timing for a hospital stay. For those that wanted to move forward but couldn’t, it probably wasn’t all that ‘elective’. Many nurses are seeing their hours cut which is not the effect you would expect from a pandemic.
Capt J Parker – Thanks for the insight. So we should expect reduced suicides and an increase in prescription drug deaths.
Todd Mora
Mar 25 2020 at 10:50am
Another thought I had was the fact that many people will have to delay retirement or return to work because of the economic fallout of the “shelter in place” orders. This impacts young people who will be looking for jobs, have student loan debt, and no accumulated wealth. I realize this is somewhat simplistic, however, it doesn’t take much to extrapolate from an individual’s point of view to a larger group impact.
My concern is that when you are reacting in almost panic mode to perceived threat, it is hard to have reasonable discussions about broader issues.
Stefano Cirolini
Mar 25 2020 at 1:30pm
One might reckon that the first to die are the oldest and more feeble. In Italy we still have more that 3,000 patients still in Intensive Care. These are much younger than the ones that already died (I read somewhere the median age is about 55). Presumably the true median age of the people who will die from the virus is lower than 80.
Robert Schadler
Mar 25 2020 at 9:08pm
The “economics of saving lives” is worth thinking through from an economics perspective. First of all, nothing “ends” death, but only delays it.
If say, a thousand people die at 80 years rather than 87 years: the use of scarce resources are shifted. Likely to more “productive” purposes. Entitlement programs pay out less and so are more sustainable.
Those sorts of issues are amenable to the tools economists qua economists can use.
I’m not entirely clear why extending life is inherently an “economics” issue. It is easy to see where many might see it as a value worthy of great effort, but not within the “science of economics.”
mark
Mar 31 2020 at 5:00am
Thanks a lot for this one, I really hoped to find sth. along those lines here (where else to turn?)! – Purely from an economist perspective, the death of octogenitarians may be a big boon for the Italian pension system and instead locking down the global travel and tourism industry kinda madness. – But then what economic value I put on feeling not guilty about grandparents suffocating to death as the hospital did run out of ventilators for all in need and thus switch off diabetic grandma Maria and life-time-smoker uncle Tony? – It is not just their 7.8 QALY saved or not. It is us having saved (some/many/half/most) of them not just from an earlier death but also from a more brutish one. Our deaths here in Germany under intensive care make me cringe less than those in Italy on the hospital corridor. So, yeah, flattening the curve has more benefits than just the QALY. And looking at the approval rates of the lock-down, most are willing to pay for this good, so it must be worth it for us. “F… the GDP” for a while. –
(But keep in mind there are costs and benefits, and there are price-tags for QALY, not all of them worth/possible paying. Sweden seems to get the balance better than Germany; we should be able to tell 3 weeks from now. And 10 months from now. Result may be: Stocking up on ventilators, masks and extra-capacity is well worth a few million € a year. Lenghty lock-downs at less than 1% mortality are not.)
Michael
Apr 9 2020 at 3:35am
https://www.thecollegefix.com/epidemiologist-coronavirus-could-be-exterminated-if-lockdowns-were-lifted/
This German epidemiologist says ‘flattening the curve’ delays herd immunity.
David
Apr 15 2020 at 7:09am
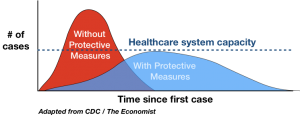
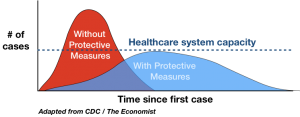
Can someone provide proof that the area under the flattened curve ( total number of deaths) is less than the area under the peaked curve (no social distancing). I don’t see it. Saving the health care system from being overwhelmed is an entirely different argument. I also never see data on actual (not estimated) lives saved.
Flattening the curve merely extends covid-19’s duration, delaying the peak. One of its consequences is a second wave— which is not speculative. By delaying herd immunity (a kind of natural vaccine) that is one health consequence. Keeping children out of school is foolish.
The hypothesis that flattening the curve saves lives is untestable since we cannot know (Hayek) how many lives would be lost w/o mitigation. The govt bureaucrats ( Fauci and Birx) love this because it means they can never be held accountable. And henceforth they can call for a quarantine whenever a health ‘crisis’ occurs.
Comments are closed.