Life-Saving Incentives: Consequences, costs and solutions to the organ shortage
By Alexander Tabarrok

An updated, 2009, version of this article can be found at Life-Saving Incentives: Consequences, Costs and Solutions to the Organ Shortage.
“Our current organ procurement system relies solely on altruism to motivate donation. Altruism is a fine thing but it is in short supply.”
Figure 1.
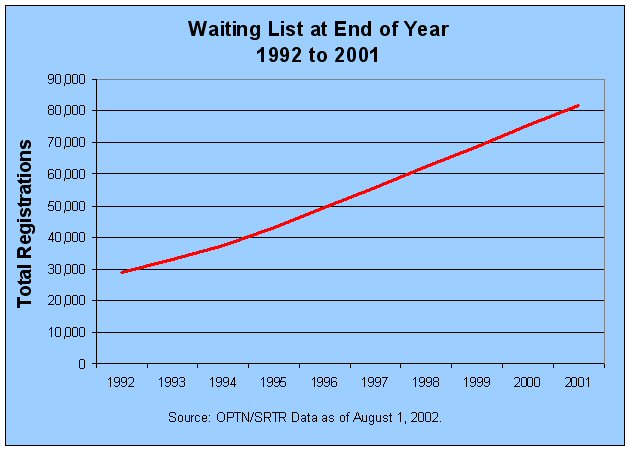
Even this higher figure is an underestimate of the deaths due to the shortage because many people who could benefit from an organ transplant are never put on the waiting list in the first place because their physicians know that the probability of obtaining an organ is low.1 The shortage of organs has other costs in addition to the deaths of those waiting for a transplant. Most obviously, the shortage greatly reduces the quality of life for those on dialysis or otherwise waiting for a transplant.
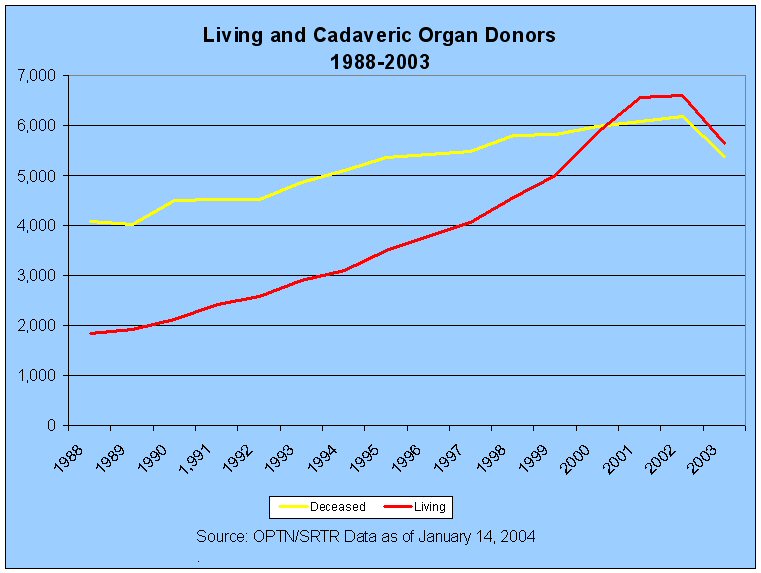
Another, rarely acknowledged cost of the shortage is the increased use of living donors. In 2001, for the first time ever, the number of living donors exceeded the number of cadaveric donors (see Figure Three).2 I greatly admire and respect all who choose to donate an organ (primarily kidneys although parts of a liver can also be donated). But it is a travesty that living bodies are medically harmed while at the same time perfectly acceptable cadaveric organs are wasted. All else being equal, reliance upon cadaveric organs is preferable to risking the health of living donors.3 If more cadaveric donations were made available, the necessity of living donations would fall.
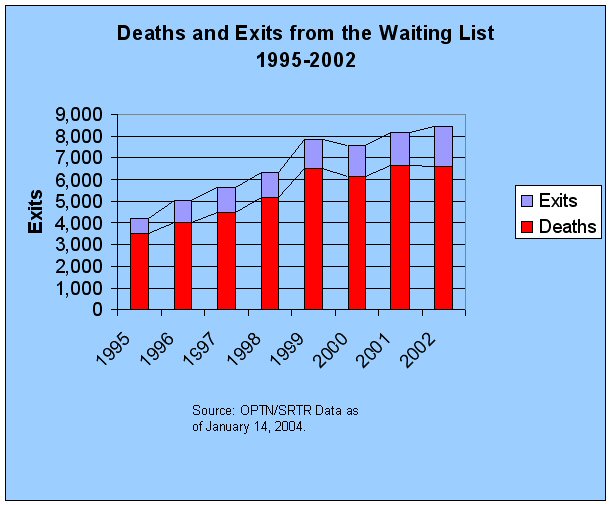
Figure 2.
Having more people on the waiting list for an organ transplant is not necessarily a bad thing, in two respects it is a sign of success. On the demand side, better surgical techniques and improved anti-rejection drugs have meant that many more people could benefit from an organ transplant if one were available. The demand for organs grows as medical knowledge advances. On the supply side, improved auto safety and a falling homicide rate have reduced the base-supply of cadaveric organs (Perez-Pena 2003). No one wants to reduce medical progress or increase the number of auto accidents, so longer waiting lists are not entirely to be bemoaned.
Nevertheless, our current organ procurement system is a terrible failure. Organs that could dramatically extend lives and return the sick to health are routinely wasted. In the United States, less than one half of potential organs donors became actual organ donors (Sheehy et al. 2003, Evans et al. 1992). The shortage of organs could be greatly alleviated, and eliminated entirely for at least some organs, if more people were to sign their organ donor cards and if more families agreed to donate after the death of a loved one.
Causes and Solutions to the Shortage
Figure 3.
Our current organ procurement system relies solely on altruism to motivate donation. Altruism is a fine thing but it is in short supply. Repeated exhortations from the government and organizations interested in organ procurement, including campaigns featuring Michael Jordan as a spokesperson, have not greatly increased organ donation in the past and are unlikely to do so in the future. We may hope for love but should plan on self-interest.
Incentives for organ donation can take a variety of forms. Financial compensation is the most discussed option but reciprocity proposals are another possibility that I discuss further below. It is currently illegal to compensate donors or their families for organ donation. To be precise, the National Organ T2ansplant Act (NOTA) of 1984 states “It shall be unlawful for any person to knowingly acquire, receive, or otherwise transfer any human organ for valuable consideration for use in human transplantation.”4
But due to the increasing shortage, support for changing NOTA is growing. The American Medical Association,The American Society of Transplant Surgeons and The United Network for Organ Sharing (UNOS) among other groups have all come out in favor of at least testing the idea of financial compensation. Congress has recently debated several bills to this effect albeit without passage Nevertheless, I predict that as the shortage of human organs grows so will support for financial compensation.
Types of Financial Incentives
In the minds of many, financial incentives for organ donation means rich people buying up kidneys being hawked on eBay by the desperately poor. In reality, we need only make marginal changes to the current system in order to create a revolution that would save many lives. Two distinctions are especially important. First, financial compensation for cadaveric donation and for living donation are different ideas and it is quite possible to have one without the other. Indeed, the primary cause of so-called organ tourism—rich people flying to poor countries like India to undergo a transplant from a poor, living donor—is the shortage of organs in the West. By allowing compensation for cadaveric donations we’ll increase the domestic supply and reduce the demand for people to fly to poorer countries for living donation. Financial compensation for cadaveric donation, in other words, is a substitute for both paid and unpaid living donation.
Second, organs are currently allocated according to a point system which is based on factors such as the quality of the match between donor and recipient, the length of time the potential recipient has been on the waiting list, the health of the potential recipient and so forth. It is not necessary to change these criteria in order to make use of financial compensation. Financial incentives can be used to increase the supply of organs without using finance to determine who will receive an organ.5
Financial incentives can be divided into forward-looking approaches and on-the-spot approaches.
Forward-thinking approaches
Forward approaches involve offering some type of incentive for people to become part of an organ donor registry so that if they die under circumstances where they can donate, their organs will be recovered. An incentive to donate, for example, could be created by something as simple as offering a discount on driver’s licenses to those who sign up to be an organ donor. Georgia, the only state with such a program, offers a discount of $9. The Georgia program has not been legally tested against NOTA, however, and the governor has said that he would like to rescind the program in order to increase state revenues (Basinger 2003).
An options market in organs would allow firms to buy the rights to organs in the event of the donor’s death (Cohen 1995, Barnett, Blair, Kaserman 1996). Every potential donor would either be paid a small amount today to join the registry or they would register today in return for the possibility of much larger payments to their estates should they become actual donors. An options market, therefore, would work much like life insurance (which used to be called “death insurance” a more accurate if less appealing name). The advantage of an options market, over an arbitrarily-chosen license fee discount or similar plan, is that firms would have an incentive to promote donation and the prices offered would automatically increase as shortages become more severe. Payments for the organs would ultimately be made by insurance companies and government just as for other medical services (see further below on the costs of financial compensation plans).
An advantage that all forward-looking approaches share is that the autonomy of the donor is maximized and the decision-making burden is taken off the family at that most difficult time, when they have just learned that their loved one is brain-dead. And, fortunately, experience shows that when families are informed of their loved one’s wishes, they almost always assent to the donation (Siminoff et al. 2001).
On-the-spot approaches
“On-the-Spot” incentives are offered only to the families of people who are suitable deceased donor candidates. The American Society of Transplant Surgeons, for example, has said that it would be ethically acceptable to offer to make a charitable contribution on behalf of the deceased or to cover the funereal expenses of deceased organ donors (Arnold et al. 2002). In my judgment, a direct payment to the estate of the deceased would also be ethically acceptable. Payments of this kind can be given as a way of saying thanks for the sacrifice the family has made in service to the community and would be similar to the death benefit offered to the families of servicemen who die in the line of duty.
For example, the Ad Hoc Committee to End the Intractable Shortage of Human Organs, of which I am a member, has recommended a gift for the gift of life that would go the estate of deceased organ donors. We have suggested that the following type of language that should be used in approaching the family of a potential donor.
Dear Mr. Smith/Ms. Jones, as you may know, it is our standard policy to offer a gift of $5,000 to the estate of the deceased, as a way of saying “Thank you for giving the gift of life.” The money can be used to help offset funeral or hospital expenses, to donate to your loved one’s favorite charity, or simply to remain with the estate, to be used in any manner the heirs see fit. No price can be placed upon the many lives that can be saved by your gift. Our donation in return is merely society’s way of honoring the sacrifice you are being asked to make, and is a token of our deep and sincere appreciation for your generosity at this most difficult time.
Saving money while saving lives
In this age of expensive medical care, many people wonder whether financial compensation for organ donation would be too expensive. In fact, we can save money while saving lives. Kidney transplants are cheaper than dialysis over prospective lifetimes and they pay for themselves within 2-3 years (Schweitzer et al. 1998, Loubeau et al. 2001, Matas and Schnitzler 2004). Most of the costs of dialysis are paid for by the Federal government through the End Stage Renal Disease (ESRD) program. Thus, any increase in organ supply automatically reduces costs to the Federal government. How much would it cost to increase donation rates from say 6000 to 9000 a year? $2500, $5000, $10,000 per donor? At $10,000 the costs of financial compensation would be $90 million but each additional kidney saves the Federal government approximately $100,000 so savings would be at least $210 million per year.6 Thus on a pure financial basis paying donors pays for itself. More importantly, increases in organ donation would allow more dialysis patients to live longer, better lives. Adding in the value of these additional quality-years would significantly increase the value of donation.
Reciprocity Plans
The economics of common resources provides another perspective on the shortage of organs. Resources owned in common tend to be under-supplied and over-utilized. No one wants to pay to restock a lake, for example, when the benefits of restocking flow to everyone regardless of whether or not they helped to pay for the restocking. As a result, open fisheries are almost always driven to depletion. The solution is to close the fishery to those who do not help to restock the lake.
UNOS considers organs to be a “national resource,” owned in common. The result, as in other areas, is a tragedy of the commons. Everyone wants to fish in the organ pool but no one has a direct incentive to “restock the lake” by signing their organ donor card. As with fishing lakes, a solution to this problem is to close the organ pool to non-donors.
Consider a no-give, no-take policy for organs (Tabarrok 2002, Gubernatis and Kliemt 2000). Under this system in order to receive an organ you must have previously signed your organ donor card.7 Under no-give, no-take, signing your organ donor card can be thought of as joining a club, the club of people who have agreed to share their organs. Or one can think of signing the organ donor card as the price that you pay for organ insurance.
An advantage of the no-give, no take policy is that it satisfies most people’s moral intuitions. Many people find the idea of paying for organs distasteful but nevertheless are comfortable with the morality of reciprocity, those who are willing to give should be the first to receive.
A variant of no-give, no-take can be implemented quite easily within the current system by giving those who have previously signed their organ donor cards extra points that would advance them on the queue. In fact, a similar program is already in place. People who have previously been live organ-donors are given extra-points should their one remaining kidney fail them. No-give, no-take simply extends this idea from actual donors to potential donors.
Something like no-give, no-take is currently being implemented privately. Lifesharers.com is an “organ club.” Anyone can join.8 Members agree that if their organs should become available they will go first to a fellow Lifesharers member. (If everyone joins Lifesharers, it becomes equivalent to no-give, no-take.)
Although reciprocity proposals like no-give, no-take have moral advantages it is important to remember that their primary purpose is to increase the incentive to donate and therefore to increase the total number of organs available.
Conclusion
Adam Smith noted that in his time there were “some very agreeable and beautiful talents of which the possession commands a certain sort of admiration; but of which the exercise for the sake of gain is considered, whether from reason or prejudice, as a sort of public prostitution.” [An Inquiry into the Nature and Causes of the Wealth of Nations, Book I, Chapter X, par. I.10.28] As examples, Smith lists acting, opera singing and dancing. Today the list strikes us as peculiar, perhaps even foolish. What could possibly make opera singing admirable when done for free but despicable when done for pay?
And yet, however peculiar the views of Adam Smith’s contemporaries were on financial compensation for opera singers we can an at least say this in their favor—no one ever died because of a shortage of singers.
Arnold, R. et al. 2002. Financial Incentives for Cadaver Organ Donation: An Ethical Reappraisal. Transplantation 73 (8):1361-67.
Basinger, B. 2003. Organ Donor Discount Could End. Savannah Morning News Feb. 06, 2003. Available at: http://www.SavannahNow.com.
Cohen, Lloyd R. 1995. Increasing the Supply of Transplant Organs: The Virtues of an Options Market. New York: Springer; Austin: R. F. Landes.
Barnett, A. H., R. D. Blair, and D. L. Kaserman. 1996. A Market for Organs. Society 33 (6):8-17. Reprinted In Entrepreneurial Economics: Bright Ideas from the Dismal Science, ed. A. Tabarrok. 2002. Oxford: Oxford University Press.
Evans, R. W., C. E. Orians, and N. L. Ascher. 1992. The Potential Supply of Organ Donors: An Assessment of the Efficacy of Organ Procurement Efforts in the United States. Journal of the American Medical Association 267 (2):239-46.
Epstein, R. A. 1993. Organ Transplants: Is Relying On Altruism Costing Lives? The American Enterprise 50 (October/November):51-57.
Gubernatis, G., and H. Kliemt. 2000. A Superior Approach to Organ Allocation and Donation. Transplantation 70 (4):699-707.
Loubeau, P. R., J. M. Loubeau, and R. Jantzen. 2001. The Economics of Kidney Transplantation Versus Hemodialysis. Prog Transplant 11 (Dec):291-97.
Matas, A. J., and M. Schnitzler. 2004. Payment for Living Donor (Vendor) Kidneys: A Cost-Effectiveness Analysis. American Journal of Transplantation 4 (2):216-21.
Perez-Pena, R. 2003. Downside to Fewer Violent Deaths: Transplant Organ Shortage Grows. The New York Times 2003 (19 August):B1.
Schweitzer, E. J. et al. 1998. The Shrinking Renal Replacement Therapy “Break-Even” Point. Transplantation 66 (8):s5.
Sheehy, E., S. L. Conrad, L. E. Brigham, R. Luskin, P. Weber, M. Eakin, L. Schkade, and L. Hunsicker. 2003. Estimating the Number of Potential Organ Donors in the United States. New England Journal of Medicine 349 (7):667-74.
Simnoff, L. A., N. Gordon, J. Hewlett, and R. M. Arnold. 2001. Factors Influencing Families’ Consent for Donation of Solid Organs for Transplantation. Journal of the American Medical Association 286:71-77.
Tabarrok, A. 2002. The Organ Shortage: A Tragedy of the Commons. In Entrepreneurial Economics: Bright Ideas from the Dismal Science, ed. A. Tabarrok. Oxford: Oxford University Press.
URREA; UNOS. 2002 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients: Transplant Data 1992-2001 [Internet]. Rockville (MD): HHS/HRSA/SPB/DOT; 2003. Available from http://www.ustransplant.org/annual_reports/ar02/ar02_main_preface.htm
Data on waiting lists and related data can be found at www.Unos.org. In 2002, 6609 people died while on the waiting list and 1844 were removed from the list for other reasons (typically because they became too sick to undergo a transplant). There are approximately 300,000 patients participating in the End Stage Renal Disease program but only about a quarter of these are on the kidney waiting list even though in a world without shortages many more would be transplant candidates.
Although the number of living donors exceeded the number of deceased donors the living donors provide only one kidney while the deceased donors may provide two kidney as well as other organs, thus the number of transplants from deceased donors still exceeds the number of transplants from living donors.
Raw figures indicate that life expectancy at 5 years for the recipient of a living donation is higher than that for a cadaveric donation by about 10 percentage points (approx. 90 versus 80 percent). The raw figures, however, do not control for other differences between recipients of living donation and recipients of cadaveric donation. Recipients of living donation tend to be younger (think parents donating to children), spend less time on the waiting list, be better educated, and richer than recipients of deceased donation (see chapter 6 of URREA (2002)) and all of these factors would tend to raise 5 year life expectancy in this group regardless of the type of donation received.
National Organ Transplant Act of 1984, 42 USC 274e S. 301.
To be clear, there may be good reasons for allowing paid compensation to living donors as well as for changing the current criteria for allocating organs (see, for example, Cohen (1995), Epstein (1993). I am not arguing against either proposal only pointing out that these proposals are distinct from financial incentives for cadaveric donation.
Matas and Schnitzler (2004) calculate that a living donor saves the US medical system $94,579 in present value. I have assumed that the savings from cadaveric donation would be similar; although life expectancy might be somewhat less for cadaveric donation (see note 3), the costs of donation to the donor are also lower.
Children could be considered automatic recipients until say their 18th birthday. A one-year waiting period could prevent people from waiting to sign their organ donor card until they became sick.
I am an advisor to Lifesharers.com.