
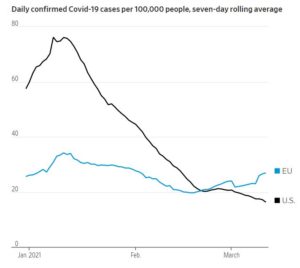
The pandemic evolution now appears to be more worrying in Europe than in America, as illustrated by the graph below reproduced from yesterday’s Wall Street Journal (Marcus Walker, Bertrand Benoit, and Stacy Meichtry, “Europe Confronts a Covid-19 Rebound as Vaccine Hopes Recede,” March 12, 2021). In France, for example, after two very long and restrictive (even tyrannical) national lockdowns, ICUs are close to 80% capacity. The Wall Street Journal explains:
Europe’s efforts continue to suffer from the EU’s slowness in procuring and approving vaccines, production delays at vaccine makers, and bureaucratic holdups in injecting available doses.
The “production delays at vaccine makers” are most likely due to the fact that the EU government has not purchased them in time while, of course, there as in America, individuals and private organizations cannot purchase them.
Those who have read Ayn Rand’s famous novel may wonder if Atlas is shrugging more visibly in Europe than in America. As for those Europeans who put all their faith in an omniscient and all-powerful welfare state, they seem deeply disappointed (although they may be asking for more). In Germany, 30% don’t trust the competence of Angela Merkel’s center-right government and trust even less her center-left parliamentary allies.
The progression of new covid variants in Europe may be an immediate culprit, but a major reason for that is that European governments, under the punctilious EU government, have been slower than the US government in making vaccines widely available to the public.
Yet, the vaccine rollout in America has not been a marvel of federal or state planning. Four months after Pfizer announced the completion of its clinical trial, three months and a half after it started delivering doses to the United States, and three months after the vaccine was approved by the FDA, only 10% of Americans are fully vaccinated and another 10% have received a first dose (according to data from the Wall Street Journal). As far as we can see, this was, although not exactly warp speed, fast enough to prevent the variants from outrunning the building of herd immunity. This relative American success was achieved with much fewer restrictions to individual liberties than in most European countries. Federalism and popular resistance have been a big advantage.
It is notable that Pfizer and its partner BioNTech were not full-fledged participants in Operation Warp Speed. Pfizer did not accept research funding to develop its vaccine. The New York Times explained (“Was the Pfizer Vaccine Part of the Government’s Operation Warp Speed?” November 10, 2020):
In July [2020], Pfizer got a $1.95 billion deal with the government’s Operation Warp Speed, the multiagency effort to rush a vaccine to market, to deliver 100 million doses of the vaccine. The arrangement is an advance-purchase agreement, meaning that the company won’t get paid until they deliver the vaccines. Pfizer did not accept federal funding to help develop or manufacture the vaccine, unlike front-runners Moderna and AstraZeneca.
Pfizer CEO Albert Bourla made that clear (see “Leading Covid-9 Vaccine Makers Pfizer and Moderna Decline Invitations to White Summit ‘Vaccine Summit’,” Stat, December 7, 2020):
Bourla later defended the decision to decline federal research and development funding, citing a desire to “liberate our scientists from any bureaucracy” and “keep Pfizer out of politics.”
Except perhaps for that, the pandemic does not provide a strong confirmation of the benefits of American free enterprise. There may be more free enterprise in America than in Europe, but it’s a matter of degree. In America too, the distribution of the vaccines has been basically a governmental affair. And think about the “price-gouging” laws that have prevented market price adjustments in 42 states, not counting the Defense Production Act at the federal level. (See Rik Chakraborti and Gavin Roberts, “Anti-Gouging Laws, Shortages, and Covid-19,” Journal of Private Enterprise 35:4 (2020), pp. 1-20.)
Perhaps the administrative-welfare state, in both Europe and America, is not as good as we thought?
READER COMMENTS
Andre
Mar 14 2021 at 8:59am
“In France, for example, after two very long and restrictive (even tyrannical) national lockdowns, ICUs are close to 80% capacity.”
What is ICU capacity supposed to be? Headlines generally appear to want to imply that ICUs should have low capacity, but I thought you’d want to run near capacity most of the time – hospitals run on thin margins and they want utilization to be high.
What is target ICU capacity at a typical hospital? I would guess around 80%, which is an approximate target for general hospital occupancy, but I’d expect someone reading this article to know.
Also, I read somewhere that (in California?) hospitals are expected/required to be able to flex to 125% of ICU capacity or somesuch. Which would mean the 100% mark is not as critical as it sounds?
A broad observation: with very very few exceptions, hospitals being overwhelmed has not been a thing with this virus. Afaict, the few exceptions were some NY hospitals last spring, maybe a few southern hospitals several months back, and some in CA more recently. All in all, it appears that way less than 1% of U.S. ICU capacity was under any kind of pressure. Quite the opposite: haven’t hospitals, on average, been far emptier than usual all year?
I’d bet that if CA hadn’t locked down for all of last year, the illness would have slow-burned and not flared as much this winter, sparing the hospital rush.
Mark Pynenburg
Mar 15 2021 at 5:33pm
In the post SARS 2003 & 2009 H1N1 era some analysis was undertaken looking at Canadian Critical Care Capacity and has some figures for the rest of the world http://www.criticalcarecanada.com/presentations/2014/canadian_critical_care_capacity.pdf
In Q1 2008/2009 Ontario teaching hospitals ICUs seem to run at an average 75% occupancy (I think that is numerical- not weighted by number of beds) with a nightly discharge average rate of 12.5% and a 48 hour re-admission average rate of 2.75%.
When hospitals hit their max occupancy they respond by increasing the rate of discharge (I assume this is an ICU discharge and not a hospital one) which in turns leads to a significant increase in re-admission to the ICU.
This paper leads me to believe that re-admission rates in the developed world are 1 in 10 during a hospitalization and are bad for patients. So Ontario teaching hospitals are doing okay at least in the first 48 hours. https://www.atsjournals.org/doi/full/10.1513/AnnalsATS.201611-851OC
The first link referenced slides from this article of 2008. https://pubmed.ncbi.nlm.nih.gov/18766102/
ICU beds per 100,000 capacity varies a lot by country and there is no standard.
From the abstract:
‘Adult intensive care unit beds also ranged seven-fold from 3.3/100,000 population in the United Kingdom to 24.0/100,000 in Germany. Volume of intensive care unit admissions per year varied ten-fold from 216/100,000 population in the United Kingdom to 2353/100,000 in Germany.’
What would be interesting would be to compare the outcome of patients who are readmitted when their discharge occurred during periods of max capacity versus similar patients who weren’t discharged, and similar patients who were readmitted when their discharge occured during periods of average capacity. An estimate of the cost in patient outcome could be weighed against the cost of increased ICU capacity. I wonder if this has already been done? I wonder if COVID-19 is leading to ICU capacities where the ICU discharge decisions of non-SARS patients are being made on these margins more often?
Mark Brophy
Mar 15 2021 at 6:29pm
Yes, CA should’ve burned away the virus slowly rather than with a winter flare. Containing the virus is like holding a beach ball underwater, eventually you’ll let go and it will pop up high. People unrealistically believe that they can suppress the virus without living on an island that can easy contain the borders.
Mm
Mar 16 2021 at 8:17am
Most EU countries have kept the number of ICU beds low by US standards as a cost containment measure-even those that have a relatively high number of “hospital beds”. “Hospital beds” is relatively meaningless if they have little resources devoted to them -they can be cheaply provided. ICU beds are another matter- tech intensive and require highly trained staff (Italy is a perfect example). Additionally, a large number of cheap hospital beds provides full employment for the nurses union.
Garrett
Mar 14 2021 at 9:15am
I think it’s too soon to declare victory on this front. A final wave driven by the UK variant is still likely before herd immunity is reached.
Pierre Lemieux
Mar 16 2021 at 9:16am
@Garrett: You are right: things can still change. But we must recall that, except perhaps in some places in California and NYC, lockdowns and other coercive measures have been more restrictive, often much more restrictive, in the EU countries than in the US.
Todd Kreider
Mar 16 2021 at 10:23am
But one can’t conclude that vaccination was that important for doing this when the increase in herd immunity was in full swing well before almost anyone was vaccinated in the U.S>
Anonymous
Mar 16 2021 at 4:37pm
You don’t think the 20% immunity from vaccination is important because we already have 30% immunity from infection? Come on, give me a break.
Todd Kreider
Mar 17 2021 at 1:44am
That isn’t what I said or Lemieux stated.
Comments are closed.