I’ve had severe allergies for as long as I can remember. Until my early-20s, I assumed I just had to live with them. Then my doctor at Princeton recommended Benadryl, which virtually cured my problem. Since then, I’ve taken antihistamines at the slightest sign of a runny nose. I’ve consumed at least 25 mg per day for over two decades. When I started hearing “Antihistamines increase dementia risk,” I was not pleased.
Despite my generic skepticism of the media’s coverage of science, I realized that if anyone was at risk, it was me. Now that I’ve finished the penultimate version of The Case Against Education, I decided to track down the original research. Here’s the full text of Gray et al.’s “Cumulative Use of Strong Anticholinergics and Incident Dementia” (JAMA Internal Medicine, 2015), and here’s the technical appendix. (All notes omitted).
Where the data come from:
This population-based prospective cohort study was conducted within
Group Health (GH), an integrated health-care delivery system in the
northwest US. Participants were from the Adult Changes in Thought (ACT)
study and details about study procedures have been detailed elsewhere.
Briefly, study participants aged 65 years and older were randomly
sampled from Seattle-area GH members. Participants with dementia were
excluded… Participants were assessed at study entry and
returned biennially to evaluate cognitive function and collect
demographic characteristics, medical history, health behaviors and
health status. The current study sample was limited to participants with
at least 10 years of GH health plan enrollment prior to study entry to
permit sufficient and equal ascertainment of cumulative anticholinergic
exposure… Of the 4,724 participants enrolled in ACT, 3,434 were eligible
for the current study…
Measuring dementia:
The Cognitive Abilities Screening Instrument (CASI) was used to screen
for dementia at study entry and each biennial study visit.
CASI scores range from 0 to 100 with higher scores indicating better
cognitive performance. Participants with CASI scores of 85 or less
(sensitivity 96.5%; specificity 92%)
underwent a standardized dementia diagnostic evaluation, including a
physical and neurological examination by a study neurologist,
geriatrician or internist, and a battery of neuropsychological testing.
Measuring drug use:
Medication use was ascertained from GH
computerized pharmacy dispensing data that included drug name, strength,
route of administration, date dispensed, and amount dispensed for each
drug. Anticholinergic use was defined as those medications deemed to
have strong anticholinergic activity as per consensus by an expert panel
of health care professionals…To create our
exposure measures, we first calculated the total medication dose for
each prescription fill by multiplying the tablet strength by the number
of tablets dispensed. This product was then converted to a standardized
daily dose (SDD) by dividing by the minimum effective dose per day
recommended for use in older adults according to a well-respected
geriatric pharmacy reference (eTable 1). For each participant, we summed the SDD for all anticholinergic
pharmacy fills during the exposure period to create a cumulative total
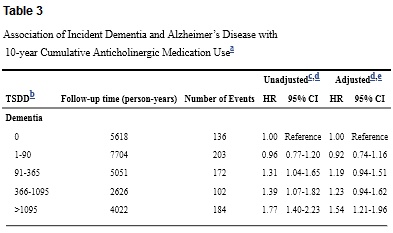
standardized daily dose (TSDD).
Here are the results for all-cause dementia, both raw and adjusted for cohort, age, sex, education, BMI, smoking, exercise, self-rated health, and a bunch of specific ailments. HR is the risk ratio; 1.31 indicates 31% elevated risk.
Overall, this is an impressive study. Yes, it only looks at seniors. Yes, there’s potential reverse causation. Yes, there are wide confidence intervals. But as far as observational studies go, it would be hard to do much better. And at least for me, the results are scary. Daily use for 3 out of 10 years puts you in the top category, with dementia risk elevated by over 50%.
As an economist as well as a Gigerenzer fan, I’m know risk ratios are a poor guide to action. I’d gladly increase my risk of being struck by lightning by 54% in exchange for one good ice cream cone. Why? Because the normal risk of being struck by lightning is minuscule. For dementia, sadly, the opposite is true. Almost one-quarter of seniors in the study ended up with dementia. But what about those big confidence intervals? They show the
danger could be much lower or much higher, but that’s all. The high
point estimates remain a reasonable guide to action.
Many will respond, “So you’re pretty likely to get dementia either way,” but that’s terrible economic reasoning. Raising the risk of losing your mind by roughly 10 percentage-points is awful – regardless of whether you’re raising the risk from 0% to 10%, 20% to 30%, or 90% to 100%. See the Allais Paradox if you’re still in doubt.
My two main initial doubts about the study:
1. While the authors brag about their dose-response function, it’s none too neat. The point estimates for low doses are negative. The point estimates for moderate doses – 95-1095 doses – are almost flat. Only the top category features a big jump. And what’s the point of these discrete categories, anyway? Why not log dosage (or dosage +1 so non-users remain in the sample), or include linear and quadratic terms? (If anyone gets the data and runs these regressions, I’ll gladly blog the results).
2. While this seems a high-quality study, publication bias is endemic; dramatic results sell. So I suspect the true effects are markedly smaller than the reported coefficients.
Reviewing the technical appendices added to my doubts. Splitting the results between antidepressants and all other anticholinigerics matters greatly. (Table reformatted for readability; all results adjusted for aforementioned controls).
With this partition, moderate use of antidepressants looks less dangerous than heavy use. And other anticholinergics just look notably safer than in the baseline results.
Patterns in eTable 5, which sub-divides results for past, recent, and continuous users, are also odd. You’d expect continuous users to do the worst, but they actually do the best. Confidence intervals are large, but still.
Given everything I’ve learned, what will I do? I definitely won’t return to my early decades of hellish allergies. Popular write-ups advise switching to second-generation drugs like Claritin. But, Claritin seems ineffective for me – and the research I’ve seen leaves its side effects unassessed.
Instead of doing anything drastic, I’m applying marginal thinking. Since serious effects aren’t evident at high doses, I’m cutting back – testing how low I can go without distress. Now that early spring is over, I’m almost asymptomatic without using any antihistamines at all. My tentative plan, then, is to limit my use to the worst allergy weeks of the year. If you’ve got better advice, please share.
P.S. Shouldn’t a Szaszian deny the reality of dementia? No. As I’ve often explained, Szaszianism is best interpreted as an empirical claim. The best way to delimit its applicability is measuring responsiveness to incentives:
The distinction between constraints and
preferences suggests an illuminating test for ambiguous cases: Can
we change a person’s behavior purely by changing his incentives?
If we can, it follows that the person was able to act differently all
along, but preferred not to; his condition is a matter of preference,
not constraint. I will refer to this as the ‘Gun-to-the-Head Test’. If
suddenly pointing a gun at alcoholics induces them to stop drinking,
then evidently sober behavior was in their choice set all along.
Conversely, if a gun-to-the-head fails to change a person’s behavior,
it is highly likely (though not necessarily true) that you are literally
asking the impossible.
Like mental retardation, and unlike alcoholism and symptoms of personality disorder, dementia seems highly unresponsive to incentives. So while I have zero worry of suddenly becoming an alcoholic, dementia really could happen to me. And I really don’t want it to…
READER COMMENTS
Philip
May 9 2016 at 9:16pm
As an allergy sufferer, I appreciate your in depth analysis on this and look forward to follow-up. Personally, I have found pollen immunotherapy to be quite effective for allergies that were not otherwise controllable with OTC medication. I still take some medication during the spring, but unlike prior to getting shots, it is actually effective.
Richard A.
May 9 2016 at 9:27pm
Durk Pearson and Sandy Shaw claim, “All of the first generation and many of the second generation antihistamines have anticholinergic effects, though not the third generation. One way to tell is if the antihistamine you use causes your mouth to become dry, it likely has anticholinergic activity.”
Peter Watt
May 10 2016 at 4:48am
Personally I’m convinced by the paleo diet ideas that argue that allergies and auto-immune disturbances are caused by modern nutrition. Too much grains causes excess omega-6 and too little omega-3 and encourages excessive inflammation. Robbwolf.com for example, explains.
EclectEcon
May 10 2016 at 7:33am
Diphenhydramine HCL, the active ingredient in Benadryl, is also the main ingredient in some over-the-counter sleep medications like “Sleep-Eze”. I’d been taking 25 or 50 mgs of this drug to help me sleep through the night for about 2-3 years when I read about this study. I immediately stopped. After all, I’m in the over 65 age group and am at high(er) risk as a result. My sleep is still messed up, but I’m hoping I’ve reduced the risk of dementia in the not-so-distant future.
ieiunus
May 10 2016 at 7:49am
[Comment removed for supplying false email address. Email the webmaster@econlib.org to request restoring this comment and your comment privileges. A valid email address is required to post comments on EconLog and EconTalk.–Econlib Ed.]
walterb
May 10 2016 at 9:33am
Re: gun to the head test, those with a dark sense of humor might seek out the Stephen King short story, “Quitters, Inc.”
August Hurtel
May 10 2016 at 10:09am
N-acetyl cysteine may well keep the runny nose at bay, and it is supposed to have a range of other good effects.
I would not be surprised if those suffering in the study were dealing with two issues- 1. the drug, and 2. a low choline diet. Mainstream recommendations tend to be against eggs and other animal products- especially in past years. A reduction of choline and the drugs over time would equal a powerful attenuation of the acetyl-choline pathway. This would be very bad for one’s ability to think at all.
RPLong
May 10 2016 at 10:25am
“dementia seems highly unresponsive to incentives”
Well, be careful. Type 2 diabetes responds to incentives, and is highly correlated with dementia.
Philo
May 10 2016 at 12:39pm
@ RPLong:
Bryan is talking about having dementia, not about getting dementia.
Mark Bahner
May 10 2016 at 1:04pm
How do the people doing the study know that it’s the drugs, not the problems that the drugs are treating, that’s causing the increased risk of dementia?
Did they find people suffering equally badly from allergies and depression, but not taking any drugs, as a control? (I realize I could just read the study, but my lunch period is almost over.)
Michael Terry
May 10 2016 at 1:37pm
I had chronic bad hay fever for as long as I could remember. As a kid, a doctor told my mom I had a line across the bridge of my nose due to the “allergist’s salute”.
Benadryl stopped working for me, but I used Zyrtec every day for years and it worked great, with no soporific effect.
However, in the last couple years–in my late 30s–at some point I cured my allergies. I had been getting regular nose bleeds, so I decided to test whether the cause was a deficiency in some essential nutrient. Since I know that multivitamins have too much of some nutrients, not enough of others, and almost always cheap forms that are not bioavailable according to research, I bought individual researched forms of every known essential nutrient and gradually started introducing them.
Vitamin C made the nosebleeds go away immediately, so I knew that supplementation could be effective, contrary to media myth. Some chronic sub-clinical deficiencies are probably pretty common.
Fascinatingly, at some point my hay fever went away also. I don’t know what caused it for sure, but it seems likely to be the supplementation. My current best guess is the scoops of soluble fiber, in the form of raw potato starch, that I started adding to my protein shakes. I’ve always hated fruits and vegetables, but the intestinal lining prefers to feed on a short chained fatty acid called butyrate that’s emitted by gut bacteria when they feed on soluble fiber. When the gut absorbs butyrate, the intestinal mesh gets tighter and healthier. We have reason to believe that a “permeable” intestinal lining is implicated in allergies, so this is what leads me to my guess.
My son has bad hay fever, so I’m planning to experiment on him to determine if supplementation will help, but I haven’t gotten around to it.
Ben H.
May 10 2016 at 1:44pm
Broadly speaking, sure; this is always a caveat when reading in the scientific (or economic, presumably) literature. In any given specific instance, the question is of course whether you actually think that previous studies on the same question were likely to have been done, produced negative results, and thus didn’t get published. It’s hard to know for sure, but in this case it seems doubtful – or at least doubtful that those prior studies would have been as thorough, with thousands of participants, etc. If somebody invests that much time and effort and money in doing a study, they generally follow through to see it published, unless they have a reason not to (such as a pharmaceutical company having a specific disincentive to publishing negative results about drugs it is developing).
Colombo
May 10 2016 at 2:01pm
I’ve used vitamin C for my allergies and it worked very well. Vitamin C supplementation, and its use as a drug at therapeutical doses is somewhat frowned upon in the paleo-diet world. Paul Jaminet does recommend vitamin C, and he is not a salesman or an activist in disguise of a scientist.
RPLong
May 10 2016 at 2:20pm
@ Philo – Right you are. My mistake.
The Original CC
May 10 2016 at 2:55pm
BC, if you’re still worried, try getting allergy shots. They changed my life. I’ve gone from being an allergy sufferer to being allergy-free.
Michael Dittmar
May 11 2016 at 4:19am
Hi,
interesting article!
I am lucky, 60 year old, never had any allergy problem
and neither my spouse and children.
I recently learned that all over sudden
in Germany medical doctors talk about an allergy pandemic situation affecting up to 30% of the population .. from far less than
10% some 20 years back (roughly)
supposed to be similar in France were I live.
Apparently, in the school of my children about 1/3 seems to have
allergy problems.
Anyway, I learned recently that fresh untreated cow milk
contains some anti allergic things and some people claim magic results. We drink such fresh cow and very tasty milk at least since 13 years and our “luck” might just be a coincidence ..
but why not trying it?
.. might be just
Casual Observer Darkly
May 11 2016 at 11:31am
The following “Bell” herbal product has worked wonders for me: “Histamine Balance”. *
I used to use Benadryl during that part of the year that caused me allergy problems, but I never liked the dry-mouth and drowsiness it caused me. Then I read an article a few years ago (sorry no citation) that indicated that the class of anti-histamines used in products like benadryl, can interfere with heart functions. Since cardiac issues are an elevated risk factor for me, that motivated me to look for alternatives and fortunately I found one that works for me. (the fairly recent report about the dementia risk factor for benadryl’s active ingredient just adds fuel to the “incentive fire.”)
* do the herbs or this particular formulation have similar or different risk factors??? I don’t know, but could find no indication thereof.
Michael Hinton
May 11 2016 at 12:14pm
I am worried about such effects as well, since I take a lot of medication to prevent migraine, including an antidepressant on the list.
I recommend experimenting with things that may have procholinergic effects, such as CDP Choline or Alpha-GPC. I’ve started taking some of the former, but not every day because it can have a depressive effect on my mood. Taking it every other day seems to avoid this.
I’m only 33, so that may be why I don’t need more since brain acetylcholine drops with age.
You might also try taking two Claritin per day since there’s evidence the dose was chosen to keep the solomesence side effect low instead of picking the dose that was most effective and generally safe.
Good luck, some of us want your brain to stick around almost as much as you do.
Maximum Liberty
May 12 2016 at 12:48pm
I suffered terrible allergies in high school, to the point that many days were triple Benadryl just to get through classes.
I switched to fexofenadine (as a generic; Allegra was the original brand, I think). It is not an anti-cholinergic drug. I switched mainly not to be sleepy. It works better for me than Benadryl because I am happier taking it as a maintenance drug, because it doesn’t make me sleepy.
Colombo
May 24 2016 at 8:31am
Hey, I just learned about this:
https://biomerestoration.com/hdc/
through this:
https://www.bulletproofexec.com/sid-baker-311/
So bizarre!
Worms with Virgin Mary’s face on them! Oh my!
HDC: Hymenolepis diminuta cysticercoides
https://en.wikipedia.org/wiki/Helminthic_therapy
They claim this is very good for allergies. Please, watch minute 46:56 of this interview: https://youtu.be/kDhB_kQjjYA
Now. All these guys of integrative medicine are clearly communists. But by studying all these parasites and bacteria they seem to be understanding **on their own** what free-market economists teach and preach about “spontaneous order”. If one of these commies could rid Bryan Caplan of his allergies, perhaps Bryan Caplan could save their poor souls from communism. Great plot for a comic book…
Comments are closed.